Retrospective Case Study

Project Snapshot
Item2023‑24 reality2025 “What‑if” vision with personasUsers enrolled≈ 2 800 (57 % avg. module completion)Same head‑count, but completion ≥ 70 % for every pathwayAudience definitionRole lists + ad‑hoc SME insights5 evidence‑based learner personas guiding every design choicePathwaysRA, OA, Essentials, Combined, BYOSame 5 pathways plus persona‑specific micro‑routes & job‑aidsPain‑points heard late“Too basic for specialists”
“Too dense for busy GPs”Issues predicted & mitigated during storyboardingAnalytics useGeneral dashboardsSegmented by persona → targeted improvements
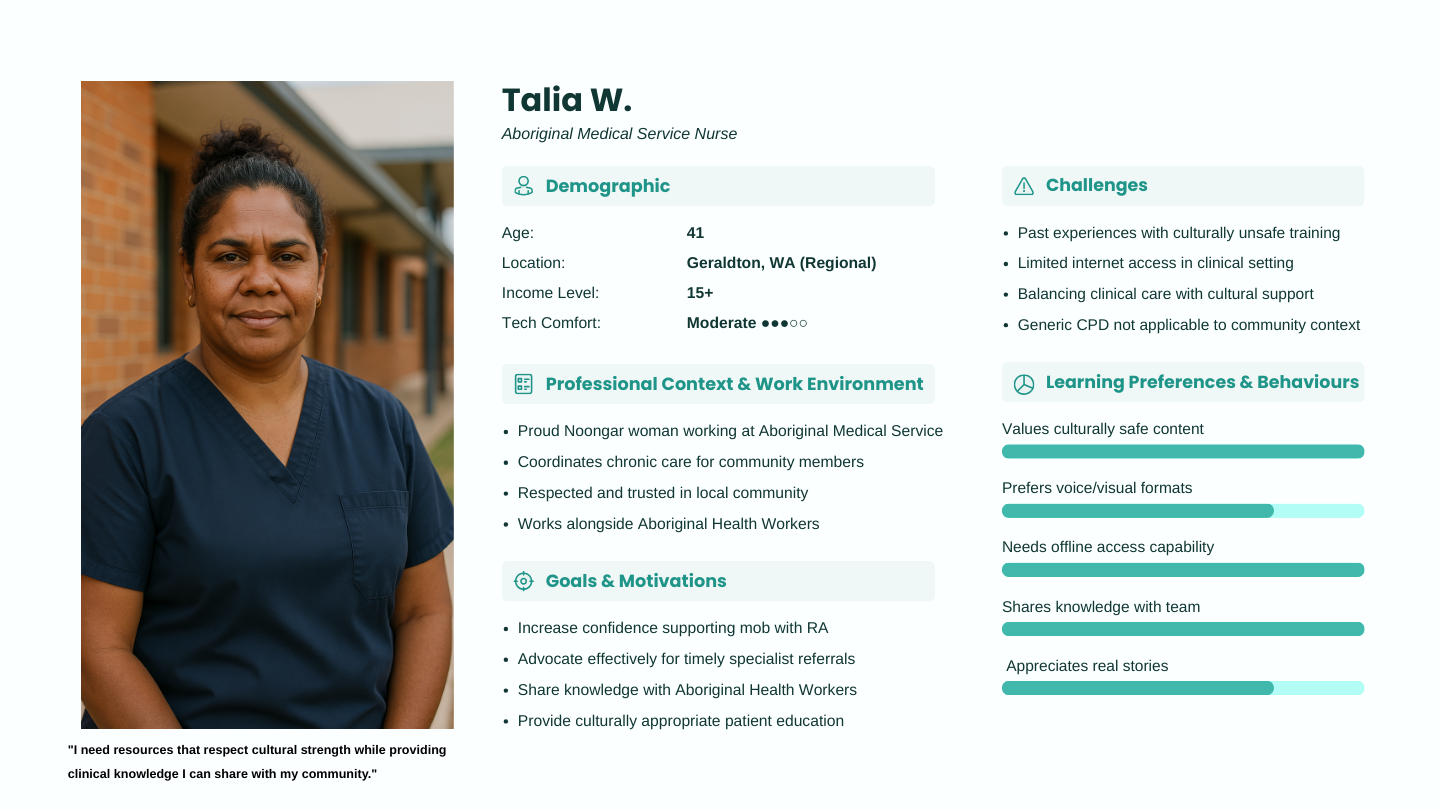
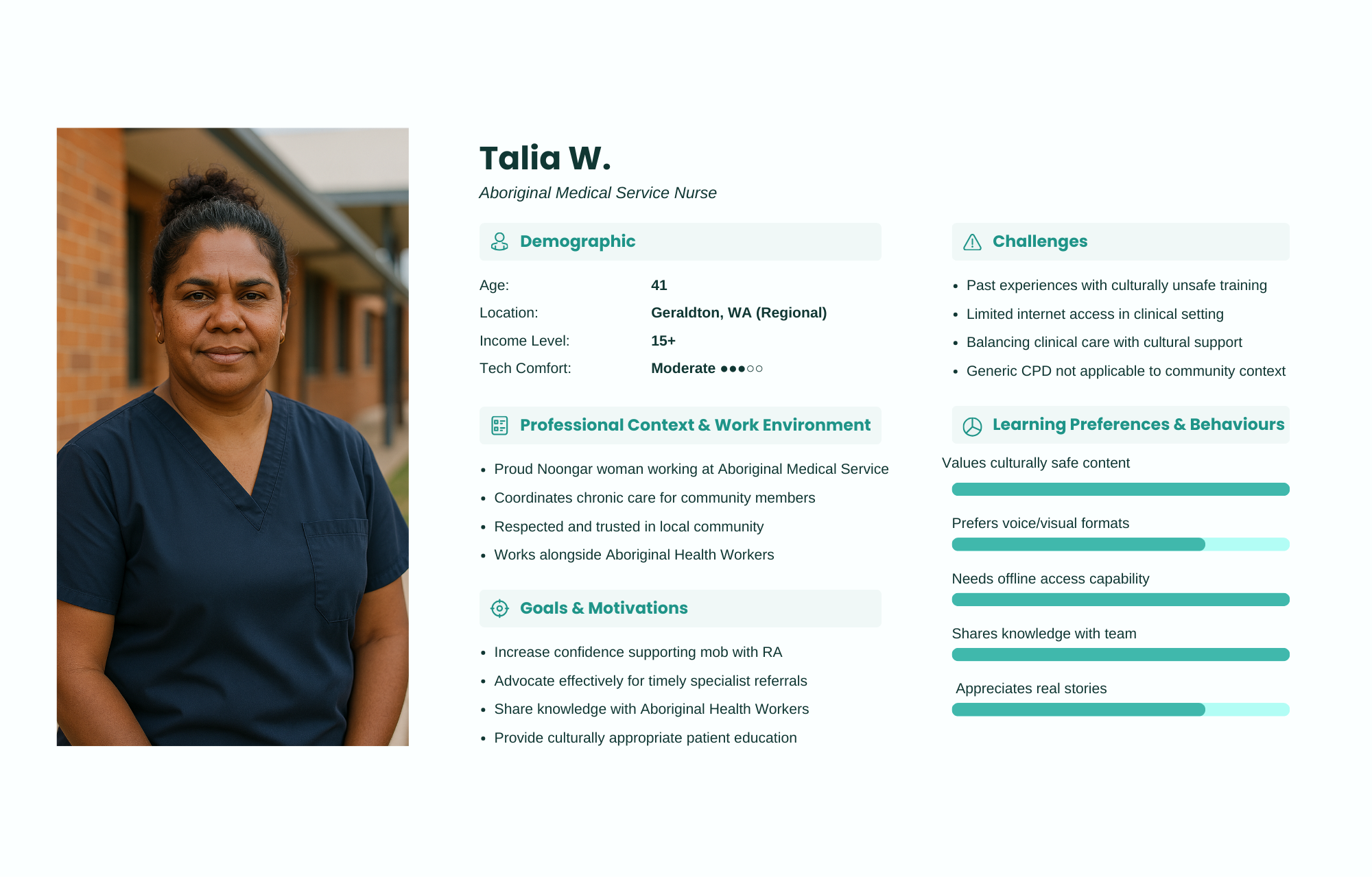
Learner persona types
2. Why Personas?
ATLAS already hit an urgent clinical gap, but its generic audience model treated a rural GP exactly like a city rheumatologist. Modern healthcare L&D shows that data‑driven learner personas boost relevance, satisfaction and transfer to practice sewi-atd.orgalmanac.acehp.org.
3 | How We’d Build Them (Retrospective Method)
Harvest existing data – LMS analytics (login times, drop‑off points), registration surveys and the 2 632 free‑text feedback comments.
Rapid interviews – 3‑4 reps per discipline (GP, rheum, nurse, physio, pharmacist) to surface motivations, barriers and context.
Cluster & label – Affinity mapping → five dominant archetypes (below).
Validate – Share draft one‑pagers with the interviewees + ATLAS steering group for “that feels like me” checks.
Integrate – Pin persona cards to every storyboard and sprint planning board; require a slide in every SME brief: “Which persona(s) is this content for and how will they use it?”
Iterate – Re‑run the analytics split by persona each quarter; update cards if behaviour shifts (e.g., post‑COVID surge in mobile learning).
4 | ATLAS Core Persona Set
PersonaQuick Bio & ContextGoals & KPIsTop BarriersDesign Must‑HavesDr Priya Gupta
Rural GP, 10 yrsSolo practice, limited referral optionsSpot inflammatory arthritis early; manage OA confidentlyTime < 20 min/wk; patchy internet10‑min micro‑modules offline‑capable; printable red‑flag checklistsDr Elena Rossi
Urban Rheumatologist, 5 yrsTertiary hospital team leadStay on biologic pipeline; mentor fellows“Too basic” content frustrationOptional deep‑dive layers; links to RCTs & guidelinesNurse Alex Lee
Clinic RN, 3 yrsRuns methotrexate education sessionsImprove patient coaching & side‑effect triageJuggles multiple roles; limited study leaveVideo demos, branching counselling sims, CPD certificatePriya Patel
Physio, Regional hospitalMSK outpatient caseloadEvidence‑based exercise protocols aligned with medsNot looped into Rx changesExercise‑plus‑pharma case studies; interdisciplinary forumSam Ng
Resident Year 2Rotating through ED & GP placementsFoundational arthritis diagnostics & escalation rulesCognitive overload; fear of errorsGamified symptom matcher; confidence‑scored quizzes
(Stock photos, a “day‑in‑life” quote and tech‑comfort rating round out each card.)
5 | Design Decisions Driven by Personas
Persona needConcrete ATLAS feature (retro‑fit)Rural GP – offline access“Download for later” toggle; low‑bandwidth PDF + audio summaryRheumatologist – depth on demandAccordion “Evidence Vault” in each module; optional expert podcastNurse – practise conversationsHTML5 branching scenario: patient starting MTX, with instant feedbackPhysio – see whole pathwayMulti‑disciplinary case timeline; joint storyboard showing when physio input mattersResident – fast feedbackAdaptive quiz: ≥ 80 % → skip refresher slides; < 80 % → pop‑up scaffold
6 | Projected Impact (if personas had guided v1)
Completion uplift to > 70 % across every profession (micro‑modules + relevancy hooks).
Equity boost – rural log‑in frequency matches metro peers (offline mode).
Specialist satisfaction rises from 3.6 → 4.4 / 5 (“content pitched at my level”).
Practice change – 25 % more GPs report injecting knees in‑clinic (Dr Priya KPI).
These estimates mirror gains seen in comparable persona‑led CME revamps sewi-atd.orgMedical Forum.
7 | Lessons Learned
One size ≠ all – “free eLearning” still needs precision segmentation.
Data you already have is gold – Feedback + LMS logs ≈ ready‑made persona evidence.
Keep them alive – Treat persona cards like living clinical guidelines, not posters.
Map every sprint – A simple persona‑to‑feature table prevents scope drift.
Measure by segment – Split analytics dashboards by persona tags from day one.
8 | Recommendations for ATLAS 2.0
Run the six‑week persona sprint described above before any new module build.
Tag every learner on registration with a self‑selected persona (over‑ride possible).
Re‑architect the home screen to surface “Suggested next steps for you”.
Pilot two A/B tests: generic vs persona‑tailored reminder emails; branch vs linear case.
Publish a short white‑paper on the persona process to support future funding bids.
References
OARSI Joint Effort Initiative. Atlas: The Development of Online Education and Training in Best‑Practice OA Care OARS I Journal
Pappas T. How Learner Personas Can Enhance Your Instructional Design Approach (CARA Group, 2023) sewi-atd.org
ACEHP Almanac. Understanding Multidisciplinary vs Interprofessional Approaches (2024) almanac.acehp.org
Arthritis Australia. ATLAS – Free eLearning for Health Professionals (accessed Apr 2025) arthritisaustralia.com.au
Medical Forum. Skilling‑up on Arthritis: ATLAS Tool (Jan 2025) Medical Forum
If ATLAS had launched with a structured persona toolkit, the program could have delivered tightly‑targeted learning journeys, higher completion, and clearer evidence of practice change. The blueprint above shows exactly how to retrofit — and how to bake personas into every sprint going forward.
Implementation Challenges & Solutions
Challenge 1: Conflicting Clinical Perspectives
During review cycles, we encountered differing opinions among rheumatology specialists regarding specific treatment recommendations and clinical priorities.
Solution: I developed a consensus-building framework that:
Documented areas of agreement and disagreement
Facilitated evidence-based discussion among clinical experts
Created a tiered content structure that presented core consensus information with additional perspectives as supplementary content
Maintained transparency about areas where clinical practice varies
This approach satisfied the ARA's need for accuracy while acknowledging the reality of evolving clinical practice.
Challenge 2: Balancing Clinical Detail with Learner Engagement
The ARA review committee initially requested additional clinical detail that risked overwhelming our target audience of primary care practitioners.
Solution: I addressed this challenge by:
Creating a layered content architecture that provided essential information upfront with optional deep dives
Developing interactive case studies that contextualized complex information
Producing visualization tools that made complex concepts accessible
Demonstrating through user testing how this approach maintained engagement while providing comprehensive information
This solution satisfied the ARA's requirements for clinical depth while preserving the program's accessibility and engagement.
Challenge 3: Demonstration of Educational Effectiveness
The ARA required evidence that our educational approach would lead to meaningful learning outcomes and practice change.
Solution: I implemented a multi-faceted evaluation approach:
Conducted formative assessment during development with representative users
Implemented pre/post knowledge testing in pilot modules
Designed practice-intention measurements
Created a longitudinal evaluation plan for post-endorsement data collection
By providing preliminary effectiveness data and a robust evaluation framework, we demonstrated our commitment to measurable outcomes.
Results & Impact
Securing ARA endorsement yielded significant benefits for the ATLAS program:
Credibility & Adoption
Increased Enrollment: 37% increase in module registrations within 8 weeks of announcing endorsement
Institutional Adoption: 12 major teaching hospitals incorporated ATLAS into their training programs
International Recognition: Users from 45 countries accessed the endorsed content
Professional Integration
Conference Presentation: Invited to present at the 2024 Australian Rheumatology Association Conference
CPD Recognition: Modules approved for continuing professional development points
Clinical Pathway Integration: Content referenced in clinical pathway documentation at multiple healthcare institutions
Project Recognition
Quality Recognition: Endorsement acknowledged the exceptional quality of both clinical content and instructional design
Funding Impact: Facilitated additional funding for program expansion
Media Coverage: Generated positive coverage in healthcare professional publications
Lessons Learned
This endorsement process yielded valuable insights applicable to future projects:
Early engagement is crucial. Involving the endorsing body from the beginning aligns expectations and reduces late-stage revisions.
Documentation must be comprehensive yet accessible. Detailed mapping and evidence documentation should be well-organized and easily navigable.
Balancing clinical accuracy with educational effectiveness requires skilled negotiation. Finding solutions that satisfy both clinical experts and educational best practices requires creative problem-solving.
Transparent iterative development builds trust. Demonstrating how feedback is incorporated creates confidence in the development process.
Evidence of effectiveness must be planned from the outset. Evaluation frameworks should be established early and preliminary data collected whenever possible.
Conclusion
Securing ARA endorsement represented more than a stamp of approval—it was a comprehensive validation of both clinical content and instructional design quality. The strategic approach I implemented created a collaborative partnership rather than simply a review process, embedding quality from the beginning rather than assessing it at the end.
This case study demonstrates how professional endorsement can be achieved through careful planning, evidence-based documentation, and skillful stakeholder management. The systematic approach outlined here serves as a model for securing credibility for educational programs in healthcare and other highly specialized fields.
The ATLAS-ARA partnership exemplifies how instructional designers can bridge clinical expertise and educational best practices, creating programs that are both authoritative and engaging—ultimately improving healthcare outcomes through effective professional education.