Managing this process end-to-end has been a valuable opportunity to develop my instructional design skills. Reflecting on my own learning throughout this experience, I have identified key takeaways that I will carry forward into future projects.
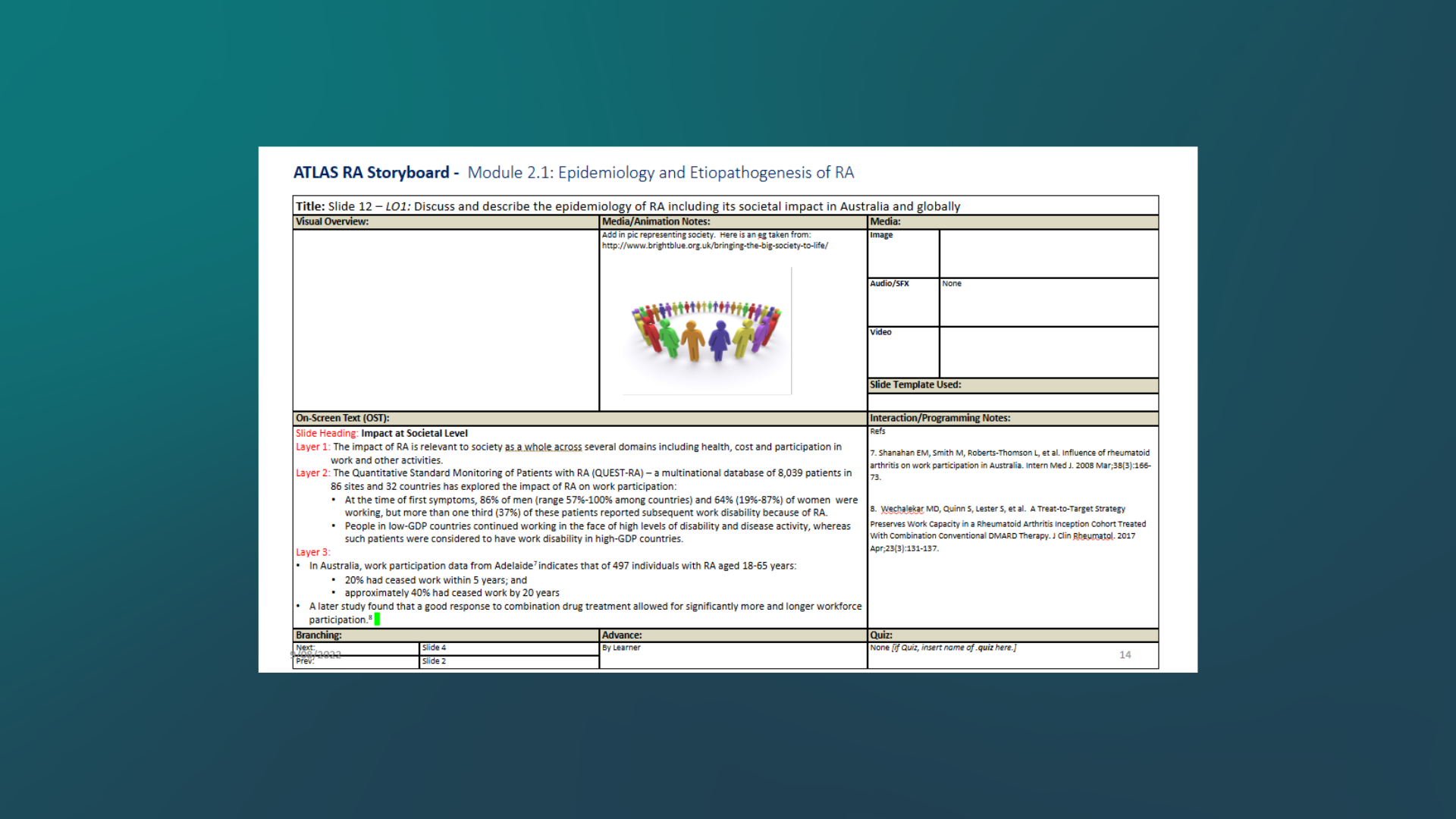
Timing is crucial: It took a lot of finessing in Vyond and Storyline 360 to ensure the animations aligned with the text prompts and moved along at a reasonable pace for the learner. A tool that helped me with this was using a stopwatch while I read the prompts to accurately estimate the time needed for each scene. I know from my own experience interacting with eLearnings that it’s a fine line finding the right pace, and I wanted to make sure I gave this extra attention to avoid a frustrating experience.
Sound and video inspiration: Though sound effects were minimal in this project, I feel the intention behind them added the dramatic tone I was seeking to the story. This has inspired me to find new ways to implement sound effects in future projects. I’m also eager to explore other authoring tools, like Captivate and Camtasia, to continue to upskill and utilize animations and video recording.
Text-based vs visual storyboard: Completing the text-based storyboard was the most challenging part of the process for me. Though I enjoy writing, I’m a visual learner, so envisioning the entire storyline through text took longer for me to complete than I initially thought. Next time, I’d like to try utilizing a different storyboard template that incorporates the visual aspect of the project as well. By doing this, my hope is that the storyboard process will be smoother and more enjoyable for me.
Appreciation for the ID process: The instructional design process consists of many steps, feedback loops, and iterations. Though I knew the process going into it, it’s a different experience when you’re head-first developing a project. It’s something that can’t be rushed and requires a thoughtful mind, an eye for detail, and patience with technology. Though some steps were more challenging than others, I absolutely loved bringing my vision for this project to life and am humbled by the work it took to get here.
Consistency across design elements is essential, especially en creating an inclusive and diverse experience.
From the start, I wanted to create characters and select graphics appealing to various backgrounds and identities. To this end, it was difficult to find graphics that were visually and stylistically consistent. This required me to create and adapt graphics and images to create the uniformity I needed from an instructional design perspective without compromising any of the valuable DEI components.
Invest time and a detail-oriented mindset in the planning and design phase to save time and effort in the development phase.
The old adage, "measure twice, cut once," speaks volumes in this context.
By refining instructional design blueprints early on, we minimised costly revisions later in the process.
Lead with curiosity.
Staying curious and committed to lifelong learning has been essential in navigating complex instructional design challenges.
Deep dives with SMEs, understanding complex business needs, and staying up to date with emerging instructional design and AI developments strengthened my problem-solving abilities.
Strong communication protocols and early collaboration with accrediting bodies are critical for success.Managing a geographically dispersed SME team taught me the importance of clear communication and culturally sensitive engagement. Navigating CPD and regulatory requirements early in the process helped avoid last-minute revisions that could have delayed the project’s launch.